

When You Have Pain “Down There” During Pregnancy …
/Imagine for a second what your life would be like without Google (scary thought, isn’t it?). If you’re a university student, you can probably attest that much of your existence relies on Google, the almighty search engine that we use to look up pretty much everything from “restaurants near me”, to song lyrics, to even ourselves (everyone has done it at least once). But, perhaps one of the most common uses of Google is to search our symptoms of something that is ailing us. If you’re like me, you’ve perfected the art of the Internet self-diagnosis. The search starts off innocent enough, but next thing you know, 20 minutes have passed and you’ve spiraled into a black hole and conclude that you may be dying.
For me, sometimes Googling my symptoms helps to alleviate these worries, and I end up feeling better knowing that whatever is afflicting me has also happened to someone else in the past. However, sometimes this fury of searching can also leave me feeling more anxious than when I started. But the bottom line here is that the Google search usually DOES have a possible explanation for our symptoms (even if we don’t like what it has to say), right?
But what if it didn’t? What if you resorted to the Internet to search for a possible explanation for your symptoms, but there was no solution? What if you didn’t see anything come up with your search? What if there was no information on the pain or symptom that you were experiencing? You might think “oh, I’ll just go see my doctor about this and it will be fine”. But what if your doctor also has no explanation for the pain you’re experiencing? What if you are otherwise physically healthy, and they have no explanation for the pain you’re experiencing?
Up until recently, this was the case for women who experienced vulvar and genital pain during pregnancy. If you typed in anything to do with “vulvar/vaginal/genital pain in pregnancy” in Google, you wouldn’t get much that popped up as a result. That’s another scary thought, isn’t it? To be pregnant and experiencing pain and not knowing how or why it’s occurring – not to mention the lack of information on the Internet that could ease your anxieties.
Thankfully, things are changing: there is a lot of work is currently being done to improve our understanding of pain experiences of women during pregnancy, and sexuality during this period more generally. As a part of a larger study at Dalhousie University [3], we wanted to get a snapshot of what women’s pain experiences were like at the half-way mark of their pregnancy (around 5 months gestation). Over 700 women who were pregnant with their first child responded to our survey.
The first question we wanted to answer: how common is genito-pelvic pain and pain during intercourse during pregnancy? * Genito-pelvic pain can be defined as pain experienced in the genital or pelvic region.
Out of 712 women, 9.1% were experiencing genito-pelvic pain. The majority of these women reported that their pain began during their pregnancy, and occurred spontaneously during certain daily activities. For women with pelvic pain, it most often occurred while sitting and walking; for women with genital pain, it most often occurred during sexual activities involving penetration.
Only 320 women answered our question on pain during intercourse, but of those who did, approximately two-thirds (66%) reported experiencing pain during sexual intercourse. It can be estimated that approximately 7-12% of non-pregnant women experience pain during intercourse [4,5], so the rates that we saw are quite a bit higher than what we would expect the see in the regular population.
Second, we wanted to answer the question of whether certain predictors (like depression or sexual distress) were associated with the presence and intensity of genito-pelvic pain and pain during intercourse.
Screen Shot 2017-10-03 at 10.26.17 AM
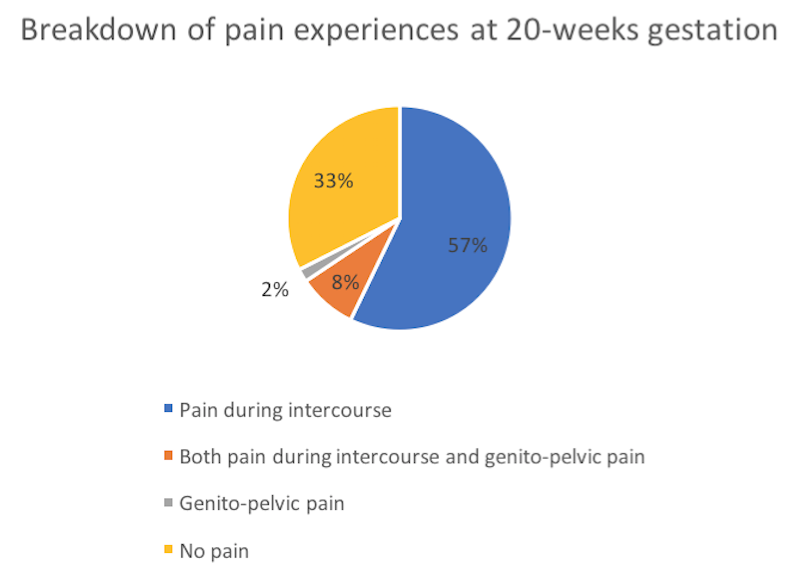
As outlined in the table above, of the 320 women who answered both measures of genito-pelvic pain and pain during intercourse …
Approximately 57% reported pain during intercourse alone
Approximately 8% of women reported both pain during intercourse and genito-pelvic pain
Approximately 2% of women reported just genito-pelvic pain
Approximately 33% of women reported neither type of pain.
Women who had higher levels of sexual distress, higher levels of depression, or higher intensity of non genito-pelvic pain were more likely to report pain (either pain during intercourse or genito-pelvic pain)
Having greater sexual distress and intensity of non genito-pelvic pain were each linked with higher pain intensity during intercourse
Greater intensity of non genito-pelvic pain also predicted (1) experiencing genito-pelvic pain and (2) genito-pelvic pain intensity.
What do these results mean? First of all, only 1/3 of participants in this study did not experience genital or pelvic pain of some sort at the half-way mark of their pregnancy. This seems like a pretty small proportion, doesn’t it? The reassuring aspect of these findings is that if you happen to be experiencing this pain, you are certainly NOT alone! The even better news is that there is preliminary evidence to show that this pain resolves for many people [6]—of course, more research needs to be done to figure out how this happens, and for whom. One thing that you can do to help? Try to find ways to reduce your pain-related anxiety.
There is evidence to suggest that pain-related anxiety (such as fear of pain, and escape/avoidance of activities that may induce pain, etc.) may worsen genito-pelvic pain symptoms in the early postpartum period [6]. If you notice that you’re worrying about painful experiences (both at present and in the future), try to identify the specific negative thoughts surrounding pain that produce anxiety or distress (for example, “the pain is terrible and I think it’s never going to get any better”); once you identify these negative thoughts, try to shift your focus to more positive internal self-statements [7]. Another suggestion is to do your best to learn more about your specific pain condition so that you can reduce the likelihood of distorting your perceptions about your own health [7]. It’s also common to experience sexual distress [8] and concerns in pregnancy [9,10], but this distress may be making your pain worse as well. Similar to what was mentioned above, identifying the specific negative sexual thoughts that are causing you distress and working to reframe these negative thoughts into positive ones may help reduce the impact of this distress on your pain experiences.
Now, these finding may seem a tad bit discouraging but the good news is that researchers out there (including some here in the SexLab) are working hard to better understand the pain experiences and sexual functioning of women during pregnancy and postpartum. Not only that, but we’re also working hard towards putting this research out in the community so that more individuals (who, like me, Google their symptoms) can more easily access the answers to their health-related questions!
Afterthought. I refer to the Internet or Google throughout this post as sources of information, but it’s very important to know where your information comes from in order to make informed judgments on the accuracy and legitimacy of the information you’re consuming. Always pay attention to the author (or authors) of an article, the author(s)’ credibility, the date of the article, the types of sources that the author cites, and the source of the information itself (e.g., institutional or governmental websites, etc.). Consult https://studyclerk.com/blog/media-literacy to learn more!
Kayla Mooney M.Sc. Student (Clinical Psychology)
[1] Bartellas, E., Crane, J. M. G., Daley, M., Bennett, K. A., & Hutches, D. (2000). Sexuality and sexual activity in pregnancy. British Journal of Obstetrics and Gynacology, 107, 964-968. doi: 10.1111/j.1471-0528.2000.tb10397.x [2] Pauleta, J. R., Pereira, N. M., & Graça, L. M. (2010). Sexuality during pregnancy. The Journal of Sexual Medicine, 7, 136-142. doi: 0.1111/j.1743-6109.2009.01538.x [3] Rossi, M., Mooney, K., Chorney, J., George, R., Pukall, C., Snelgrove-Clarke, E., & Rosen, N. O. (in prep.). Prevalence and predictors of dyspareunia and genito-pelvic pain in women 18-24 weeks pregnant. [4] Harlow, B. L., Kunitz, C. G., Nguyen, R. H., Rydell, S. A., Turner, R. M., & Maclehose, R. F. (2014). Prevalence of symptoms consistent with a diagnosis of vulvodynia: Population based estimates from 2 geographical regions. American Journal of Obstetrics and Gynecology, 210, 40.e1-40.e8. doi:10.1016/j.ajog.2013.09.033 [5] Harlow, B. L., Wise, L. A., & Stewart, E. G. (2001). Prevalence and predictors of chronic lower genital tract discomfort. American Journal of Obstetrics and Gynecology, 185, 545-550. doi:10.1067/mob.2001.116748 [6] Glowacka, M., Rosen, N., Chorney, J., Snelgrove-Clarke, E., & George, R. B. (2014). Prevalence and predictors of genito-pelvic pain in pregnancy and postpartum: The prospective impact of fear avoidance. The Journal of Sexual Medicine, 11, 3021-3034. doi: 10.1111/jsm.12675 [7] Gatchel, R. J. & Neblett, R. (2017, April 12). Pain Catastrophizing: What Clinicians Need to Know. Practical Pain Management. Retrieved from https://www.practicalpainmanagement.com/pain/other/co-morbidities/pain-catastrophizing-what-clinicians-need-know [8] Vannier, S. A. & Rosen, N. O. (2017). Sexual distress and sexual problems during pregnancy: Associations with sexual and relationship satisfaction. The Journal of Sexual Medicine. [9] Beveridge, J. K., Vannier, S. A., & Rosen, N. O. (2017). Fear-based reasons for not engaging in sexual activity during pregnancy: Associations with sexual and relationship well-being. Journal of Psychosomatic Obstetrics & Gynecology. doi: 10.1080/0167482X.2017.1312334 [10] Schlagintweit, H., Bailey, K. & Rosen, N. O. (2016). A new baby in the bedroom: Frequency and severity of postpartum sexual concerns and their associations with relationship satisfaction in new parent couples. The Journal of Sexual Medicine. doi:10.1016/j.jsxm.2016.08.006.